|
Overview
 ?Life begins at 40,? goes an old quote, ?and so do fallen arches.? It?s time to toss that negative idea out the window and get the real facts on fallen arches and what you can do about them. We have all seen what our footprints look like as we walked across sand or left a water trail after getting out of the bathtub. The narrow part of the footprint is where your natural arch exists. What gives you that arch are tendons that pull together to create an upward curve. When your tendons are not properly pulling together, you start to lose that natural arch. This condition is known as flat foot or fallen arch. Causes There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape. At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side. Symptoms Flat feet can cause a myriad of symptoms, from experiencing pain in the foot, heels, arch, calves, the shin, the knee, the hip and into the lower back due to overworking of the hip flexors or they may find it hard to stand on tip toes. Diagnosis Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis. fallen arches exercises Non Surgical Treatment If fallen arches are not causing any pain or discomfort, then they will not need any treatment. If they were causing a persistent pain in the feet, or in the hips, legs or knees, then it would be best to consult your family doctor. Walking is the natural activity of feet and if it is not too painful, sufferers should walk as much as possible to strengthen their arches. When it is possible, go barefoot, or wear soft flexible shoes. In cases of severe fallen arches, your doctor may recommend special shoe inserts. Surgical Treatment  A better approach is to strengthen the weakened ligaments with Prolotherapy, supplemented by an arch support if the condition has existed for several years. Chronic pain is most commonly due to tendon and ligament weakness, or cartilage deterioration. The safest and most effective natural medicine treatment for repairing tendon, ligament and cartilage damage is Prolotherapy. In simple terms, Prolotherapy stimulates the body to repair painful areas. It does so by inducing a mild inflammatory reaction in the weakened ligaments and cartilage. Since the body heals by inflammation, Prolotherapy stimulates healing. Prolotherapy offers the most curative results in treating chronic pain. It effectively eliminates pain because it attacks the source: the fibro-osseous junction, an area rich in sensory nerves. What?s more, the tissue strengthening and pain relief stimulated by Prolotherapy is permanent. After Care Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon. Overview
A difference in the length of your lower and/or upper legs is called a leg length discrepancy. This is fairly common, actually. One study reported that 32 percent of 600 individuals had a difference in their leg lengths ranging from one-fifth to three-fifths of an inch. A person might not even notice if one leg is slightly longer than the other. However, if the difference is not minimal, treatment may be required.  Causes A patient?s legs may be different lengths for a number of reasons, including a broken leg bone may heal in a shorter position, particularly if the injury was severe. In children, broken bones may grow faster for a few years after they heal, resulting in one longer leg. If the break was near the growth center, slower growth may ensue. Children, especially infants, who have a bone infection during a growth spurt may have a greater discrepancy. Inflammation of joints, such as juvenile arthritis during growth, may cause unequal leg length. Compensation for spinal or pelvic scoliosis. Bone diseases such as Ollier disease, neurofibromatosis, or multiple hereditary exostoses. Congenital differences. Symptoms The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship. Diagnosis Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue. Non Surgical Treatment Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.  shoe lifts for men's shoes Surgical Treatment For discrepancies over five centimeters, more aggressive surgical procedures-specifically leg lengthening procedures-are typically required. The specifics of this operative procedure are beyond the scope of this informational page, but your child's physician will be able to discuss the details in reference to your child's specific problems when considered appropriate. Overview
 You are at an increased risk of gradual wear and tear damaging your plantar fasciitis if you are overweight or obese - if you have a body mass index (BMI) of 30 or over, you are considered to be obese, have a job that involves spending long periods of time standing, wear flat-soled shoes - such as sandals or flip flops. Less common causes of heel pain are described below. A stress fracture can occur if your heel bone is damaged during an injury. Fat pad atrophy is where the layer of fat that lies under the heel bone, known as the fat pad, starts to waste away due to too much strain being placed on the pad. Women who wear high-heeled shoes for many years have an increased risk of developing fat pad atrophy. Bursitis is inflammation of one or more bursa (small fluid-filled sacs under the skin, usually found over the joints and between tendons and bones). It's possible to develop bursitis anywhere inside the body, not just in the foot. Tarsal tunnel syndrome. The nerves in the sole of your foot pass through a small tunnel on the inside of the ankle joint, known as the tarsal tunnel. If a cyst forms or the tunnel is damaged, the nerves can become compressed (squashed). This can cause pain anywhere along the nerve, including beneath your heel. Sever's disease is a common cause of heel pain in children. It's caused by the muscles and tendons of the hamstrings and calves stretching and tightening in response to growth spurts. The stretching of the calf muscle pulls on the Achilles tendon. This pulls on the growing area of bone at the back of the heel (growth plate), causing pain in the heel. The pain is further aggravated by activities such as football and gymnastics. The pain often develops at the side of the heel, but can also be felt under the heel. Calf and hamstring stretches and, if necessary, heel pads are usually effective treatments for Sever's disease. Bone spurs are an excess growth of bone that forms on a normal bone. Bone spurs can develop on the heel (a heel spur) and are more common in people with heel pain. However, they can also occur in people without heel pain. A heel spur does not cause heel pain. Causes Plantar Fasciitis is the most common form of heel pain. The tears and inflammation that develop along the plantar fascia ligament result in dull aching pain or a burning sensation along the bottom of the foot. Pain becomes particularly noticeable after periods of rest, such as during the first few steps after getting out of bed in the morning, or after getting up after a prolonged period of sitting. Another common form of heel pain is the development of a heel spur. A heel spur, as mentioned above, is the formation of a bony hook extending from the heel. Typically, these growths develop near the area where the plantar fascia connects to the heel bone. The repetitive pressure on the plantar fascia that results from stretching excessively away from the heel bone causes a response from our body that delivers calcium to the area. The heel pain that ensues develops from the nerves and sensitive tissue that become irritated when the bone fragment digs into the bottom of the heel. Pain may decrease after walking as the tissue in the heel gets used to the fragment and adjusts around it. However, pain will be particularly problematic following periods of rest. Strained muscle tissue may cause heel pain in several areas. A tight plantar fascia causes additional tension, particularly while exercising, placing runners and other athletes at risk if the ligament is not properly warmed up prior to exercise. Additionally, a tight Achilles tendon along the back of the foot can also add tension along the plantar fascia, resulting in possible damage, not to mention the damage and pain that can occur along the Achilles tendon itself (Achilles tendonitis). It is recommended that athletes properly stretch the foot as well as the calf in order to reduce tension on muscle and other tissue in the foot. Symptoms Pain typically comes on gradually, with no injury to the affected area. It is frequently triggered by wearing a flat shoe, such as flip-flop sandals. Flat footwear may stretch the plantar fascia to such an extent that the area becomes swollen (inflamed). In most cases, the pain is under the foot, toward the front of the heel. Post-static dyskinesia (pain after rest) symptoms tend to be worse just after getting out of bed in the morning, and after a period of rest during the day. After a bit of activity symptoms often improve a bit. However, they may worsen again toward the end of the day. Diagnosis After you have described your foot symptoms, your doctor will want to know more details about your pain, your medical history and lifestyle, including. Whether your pain is worse at specific times of the day or after specific activities. Any recent injury to the area. Your medical and orthopedic history, especially any history of diabetes, arthritis or injury to your foot or leg. Your age and occupation. Your recreational activities, including sports and exercise programs. The type of shoes you usually wear, how well they fit, and how frequently you buy a new pair. Your doctor will examine you, including. An evaluation of your gait. While you are barefoot, your doctor will ask you to stand still and to walk in order to evaluate how your foot moves as you walk. An examination of your feet. Your doctor may compare your feet for any differences between them. Then your doctor may examine your painful foot for signs of tenderness, swelling, discoloration, muscle weakness and decreased range of motion. A neurological examination. The nerves and muscles may be evaluated by checking strength, sensation and reflexes. In addition to examining you, your health care professional may want to examine your shoes. Signs of excessive wear in certain parts of a shoe can provide valuable clues to problems in the way you walk and poor bone alignment. Depending on the results of your physical examination, you may need foot X-rays or other diagnostic tests. Non Surgical Treatment Treatment of plantar fasciitis begins with first-line strategies, which you can begin at home. Stretching exercises. Exercises that stretch out the calf muscles help ease pain and assist with recovery. Avoid going barefoot. When you walk without shoes, you put undue strain and stress on your plantar fascia. Ice. Putting an ice pack on your heel for 20 minutes several times a day helps reduce inflammation. Place a thin towel between the ice and your heel; do not apply ice directly to the skin. Limit activities. Cut down on extended physical activities to give your heel a rest. Shoe modifications. Wearing supportive shoes that have good arch support and a slightly raised heel reduces stress on the plantar fascia. Medications. Oral nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, may be recommended to reduce pain and inflammation. Surgical Treatment With the advancements in technology and treatments, if you do need to have surgery for the heel, it is very minimal incision that?s done. And the nice thing is your recovery period is short and you should be able to bear weight right after the surgery. This means you can get back to your weekly routine in just a few weeks. Recovery is a lot different than it used to be and a lot of it is because of doing a minimal incision and decreasing trauma to soft tissues, as well as even the bone. So if you need surgery, then your recovery period is pretty quick. hold loose high heeled shoes Prevention  Heel pain is commonly caused from shoes that do not fit properly. In addition, shoes need to have ample cushioning and support, particularly through the heel, ball of the foot, and arch. Shoes should also be replaced if they become too worn. One sure sign of wear and tear is overly worn areas of a shoe's insoles. If the heel or ball of the foot is particularly worn, damage could easily occur since the bottom of the foot is not getting the cushioning it needs. Overview
 Mortons Neuroma is a common painful condition involving compression of nerves between the long bones of the forefoot just before they enter the toes. Commonly this involves the 3rd and 4th toes, however may affect the 2nd and 3rd toes. Repeated trauma or compression of these nerves causes the nerves to swell and thicken causing a Morton's neuroma to develop. Mortons Neuroma is a common painful condition involving compression of nerves between the long bones of the forefoot just before they enter the toes. Commonly this involves the 3rd and 4th toes, however may affect the 2nd and 3rd toes. Repeated trauma or compression of these nerves causes the nerves to swell and thicken causing a Morton's neuroma to develop.Causes Occupational hazards. Individuals whose jobs place undue stress on their forefeet (with or without wearing improper footwear) are among those who complain of neuromas. Podiatric physicians report that individuals who work on ladders, or who perform activities on their knees (such as doing landscaping, carpeting, flooring, or other work on the ground) are at risk for this problem, too, since these activities cause stress to the nerve near the ball of the foot. Those who engage in high-impact activities that bring repetitive trauma to the foot (running, aerobics, etc.) have a better than average chance of developing a neuroma at the site of a previous injury. To put it more simply, if you have sustained a previous injury to your foot (a sprain, stress fracture, etc.), that area of your foot will be more prone to neuroma development than an area that has not been injured. However, sports injuries aren?t automatically a ticket to neuromas. Trauma caused by other forms of injury to the foot (dropping heavy objects, for example) can also cause a neuroma to develop at the site of the previous injury. Much though we hate to say it, sometimes neuromas just develop and nobody knows why. The patient doesn?t have a previous injury, is wearing properly fitted shoes, and doesn?t stress his/her feet with any specific activity but the neuroma develops anyway. It is important to remember that some of the factors listed above can work alone, or in combination with each other, to contribute to the formation of neuroma. Symptoms The symptoms of Morton?s Neuroma tend to come and go over time. They are typically exacerbated by physical activity or by wearing certain shoes. Morton?s Neuroma symptoms include sharp pain in the ball of the foot, pain radiating to the tips of the toes, burning pain in the second, third, or fourth toes, numbness in the toes, sensation of a lump between the toes. Diagnosis Morton's neuroma is usually diagnosed by your doctor listening to your symptoms and examining your foot. Sometimes your doctor can feel the 'neuroma', or an area of thickening in your foot, which may be tender. Sometimes, your doctor may suggest an ultrasound scan or MRI scan to confirm the diagnosis but this is not always necessary. Some doctors inject a local anaesthetic into the area where you are experiencing pain. If this causes temporary relief of pain, burning and tingling, it can sometimes help to confirm the diagnosis and show the doctor where the problem is. Non Surgical Treatment You may need a metatarsal pad if wider shoes do not help relieve your Morton?s neuroma symptoms. A metatarsal pad will help spread your metatarsal bones and reduce pressure on your affected nerve as it travels under the ball of your foot. The placement of your metatarsal pad is important, and it is best placed by a foot care professional who has experience in the anatomy of the forefoot and Morton?s neuroma treatment.  Surgical Treatment When conservative measures are unsuccessful, surgery can be a good choice in the treatment of Morton's neuroma. The operation for Morton's neuroma does not require an overnight hospital stay. The anesthetic used is an ankle block, which completely numbs the foot during the surgery. The physician removes the neuroma from an incision made on the top of the foot between the involved metatarsal heads. The nerve to the interspace is exposed and cut next to the metatarsal heads. Prevention It is not always possible to prevent a Morton's neuroma. However, you probably can reduce your risk by wearing comfortable shoes that have low heels, plenty of toe space and good arch support. There are two different kinds of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is anatomically shorter in comparison to the other. As a result of developmental periods of aging, the brain senses the stride pattern and identifies some variance. The human body typically adapts by dipping one shoulder over to the "short" side. A difference of under a quarter inch is not really irregular, require Shoe Lifts to compensate and mostly doesn't have a profound effect over a lifetime.
 Leg length inequality goes mainly undiagnosed on a daily basis, yet this condition is simply solved, and can eliminate quite a few cases of lower back pain. Therapy for leg length inequality typically consists of Shoe Lifts. These are generally economical, normally being below twenty dollars, in comparison to a custom orthotic of $200 or even more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe. Lower back pain is easily the most widespread health problem afflicting men and women today. Around 80 million people are affected by back pain at some stage in their life. It's a problem that costs companies huge amounts of money every year on account of time lost and productivity. New and more effective treatment solutions are constantly sought after in the hope of decreasing the economical influence this condition causes.  People from all corners of the earth suffer from foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts can be of beneficial. The lifts are capable of eliminating any discomfort and pain in the feet. Shoe Lifts are recommended by countless qualified orthopaedic doctors. So as to support the body in a nicely balanced manner, your feet have a crucial job to play. Irrespective of that, it can be the most overlooked region in the human body. Some people have flat-feet meaning there is unequal force exerted on the feet. This will cause other parts of the body including knees, ankles and backs to be impacted too. Shoe Lifts make sure that proper posture and balance are restored.  Overview A heel spur is an overgrowth of bone that resembles a hook on the bottom of the foot. It is a reaction to stress placed on the thick connective tissue on the bottom of the foot (plantar fascia) that helps maintain the arches of the foot. Over-stress can stem from improper support of the feet. A heel spur is often accompanied by a bursitis that is a major contributor to pain. Causes These bony protrusions are commonly found in association with a condition called Plantar Fasciitis. Plantar Fasciitis occurs when the plantar fascia ligament, which spans the arch of the foot, becomes stressed, torn and inflamed. Misalignment and excessive movement of the plantar fascia ligament is most typically the result of an abnormal walking gait. The ligament is designed to stretch with the bounce of each step you take, but if it stretches too much, the resulting small tears and inflammation can cause mild to extreme discomfort. At the same time, it is believed that heel spurs are formed as the body attempts to provide some additional support to the over-stretched ligament. In other words, calcium builds up as a prop to the plantar fascia.  Symptoms Symptoms may be similar to those of plantar fasciitis and include pain and tenderness at the base of the heel, pain on weight bearing and in severe cases difficulty walking. The main diagnosis of a heel spur is made by X-ray where a bony growth on the heel can be seen. A heel spur can occur without any symptoms at all and the athlete would never know they have the bony growth on the heel. Likewise, Plantar fasciitis can occur without the bone growth present. Diagnosis Sharp pain localized to the heel may be all a doctor needs to understand in order to diagnose the presence of heel spurs. However, you may also be sent to a radiologist for X-rays to confirm the presence of heel spurs. Non Surgical Treatment A conventional treatment for a heel spur is a steroid injection. This treatment, however, isn?t always effective because of the many structures in the heel, making it a difficult place for an injection. If this treatment goes wrong, it can make the original symptoms even worse. Another interesting means of treatment is Cryoultrasound, an innovative electromedical device that utilizes the combination of two therapeutic techniques: cryotherapy and ultrasound therapy. Treatments with Cryoultrasound accelerate the healing process by interrupting the cycle and pain and spasms. This form of therapy increases blood circulation and cell metabolism; it stimulates toxin elimination and is supposed to speed up recovery. Surgical Treatment Sometimes bone spurs can be surgically removed or an operation to loosen the fascia, called a plantar fascia release can be performed. This surgery is about 80 percent effective in the small group of individuals who do not have relief with conservative treatment, but symptoms may return if preventative measures (wearing proper footwear, shoe inserts, stretching, etc) are not maintained. Prevention There are heel spur prevention methods available in order to prevent the formation of a heel spur. First, proper footwear is imperative. Old shoes or those that do not fit properly fail to absorb pressure and provide the necessary support. Shoes should provide ample cushioning through the heel and the ball of the foot, while also supporting the arch. Wearing an orthotic shoe insert is one of the best ways to stretch the plantar fascia and prevent conditions such as heel spurs. Stretching the foot and calf is also helpful in preventing damage. Athletes in particular should make sure to stretch prior to any physical activity. Stretching helps prevent heel spurs by making tissue stronger as well as more flexible. In addition, easing into a new or increasingly difficult routine should be done to help avoid strain on the heel and surrounding tissue.  Overview A heel spur is a hook of bone that can form on the heel bone of the foot. Heel spurs are associated with plantar fasciitis. Heel spurs can cause extreme pain in the rearfoot. The pain is most intense while standing or walking. What Causes Heel Spurs? Heel spurs develop as an abnormal growth in the heel bone due to calcium deposits that form when the plantar fascia stretches and pulls away from the heel. The plantar fascia is a ligament located at the bottom of your foot. This stretching of the plantar fascia is usually the result of flat feet or unusually high arches. Causes Heel spurs develop as an abnormal growth in the heel bone due to calcium deposits that form when the plantar fascia pulls away from the heel. This stretching of the plantar fascia is usually the result of over-pronation (flat feet), but people with unusually high arches (pes cavus) can also develop heel spurs. Women have a significantly higher incidence of heel spurs due to the types of footwear often worn on a regular basis.  Symptoms Most heel spurs cause no symptoms and may go undetected for years. If they cause no pain or discomfort, they require no treatment. Occasionally, a bone spur will break off from the larger bone, becoming a ?loose body?, floating in a joint or embedding itself in the lining of the joint. This can cause pain and intermittent locking of the joint. In the case of heel spurs, sharp pain and discomfort is felt on the bottom of the foot or heel. Diagnosis The proper diagnosis of a heel spur often requires an X-ray. To make this process as convenient for his patients as possible, most clinics have an on-site digital X-ray and diagnostic ultrasound machines. This can make it unnecessary for patients to visit diagnostic imaging centers, allowing patients to receive more expedient treatment. Non Surgical Treatment Heel spurs and plantar fasciitis are treated by measures that decrease the associated inflammation and avoid reinjury. Local ice applications both reduce pain and inflammation. Physical therapy methods, including stretching exercises, are used to treat and prevent plantar fasciitis. Anti-inflammatory medications, such as ibuprofen or injections of cortisone, are often helpful. Orthotic devices or shoe inserts are used to take pressure off plantar spurs (donut-shaped insert), and heel lifts can reduce stress on the Achilles tendon to relieve painful spurs at the back of the heel. Similarly, sports running shoes with soft, cushioned soles can be helpful in reducing irritation of inflamed tissues from both plantar fasciitis and heel spurs. Infrequently, surgery is performed on chronically inflamed spurs. Surgical Treatment Surgery is used a very small percentage of the time. It is usually considered after trying non-surgical treatments for at least a year. Plantar fascia release surgery is use to relax the plantar fascia. This surgery is commonly paired with tarsal tunnel release surgery. Surgery is successful for the majority of people. Overview
Bursitis (ber-SEYE-tis) is swelling and pain of a bursa. A bursa is a fluid-filled sac that acts as a cushion or shock absorber between a tendon and a bone. A tendon is a cord of tough tissue that connects muscles to bones. Normally a bursa has a small amount of fluid in it. When injured, the bursa becomes inflamed (red and sore) and may fill with too much fluid. Achilles (ah-KIL-eez) tendon bursitis is a type of ankle bursitis when the bursa between the Achilles tendon and the heel becomes inflamed. You may have Achilles bursitis and tendonitis (inflamed tendon) at the same time. Causes Systemic diseases such as rheumatoid arthritis, ankylosing spondylitis, reactive arthritis, psoriatic arthritis, scleroderma, systemic lupus erythematosus, pancreatitis, Whipple disease, oxalosis, uremia, hypertrophic pulmonary osteoarthropathy, and idiopathic hypereosinophilic syndrome have also been associated with bursitis. Symptoms What are the symptoms of heel bursitis? pain, swelling, tenderness, redness, and/or warmth at either the bottom of the heel or top of the heel, depending on the degree of swelling, pain may be a dull ache or substantial enough to cause limping, running, jumping, and walking activities may exacerbate pain, wearing poorly fitting, tight, or high-heeled shoes may exacerbate pain. Diagnosis Careful examination by your physician or physiotherapist can determine if the inflammation is from the Achilles tendon or from the retrocalcaneal bursa. Tenderness due to insertional Achilles tendinitis is normally located slightly more distal where the tendon inserts into the back of the heel, whereas tenderness caused by the retrocalcaneal bursa is normally palpable at the sides of the distal Achilles tendon. Diagnosis can be confirmed with an ultrasound investigation, MRI or CT scan. Non Surgical Treatment The underlying cause of the bursitis must be identified to prevent further reoccurrences. Failure to eliminate the cause will lead to future flare ups and a poor and slow recovery. Future occurrences can be prevented with the use of stretches and strengthening exercises which will help prevent the muscles from tightening up over the bursa, Pilates and yoga are very good for this providing the aggravating movements are avoided. Wearing joint supports such as knee pads or elbow supports may also reduce the likelihood of redeveloping bursitis. Surgical Treatment Only if non-surgical attempts at treatment fail, will it make sense to consider surgery. Surgery for retrocalcanel bursitis can include many different procedures. Some of these include removal of the bursa, removing any excess bone at the back of the heel (calcaneal exostectomy), and occasionally detachment and re-attachment of the Achilles tendon. If the foot structure and shape of the heel bone is a primary cause of the bursitis, surgery to re-align the heel bone (calcaneal osteotomy) may be considered. Regardless of which exact surgery is planned, the goal is always to decrease pain and correct the deformity. The idea is to get you back to the activities that you really enjoy. Your foot and ankle surgeon will determine the exact surgical procedure that is most likely to correct the problem in your case. But if you have to have surgery, you can work together to develop a plan that will help assure success.  Overview OverviewWhen a person has hammertoes, the end of their toe bends downward and the middle joint curls up. Eventually, the toe gets stuck in a stiff, claw-like position. When the inside of your shoe rubs against a hammer toe, corns, blisters or calluses may form on top of the toe or on the bottom of your foot. This can make walking painful. You may also have pain in the joint where your big toe joins your foot. Hammer toe usually affects a person?s second toe (the toe next to the big toe), but it can affect other toes too. Causes Those fashionable shoes. Women tend to cram their feet into too-narrow, ill-fitting shoes with little to no arch support. That?s why we see more hammertoes in women than men. Pointy, high-heeled shoes put severe pressure on the toes and their joints, and they typically have little to no arch support. Neuromuscular diseases can contribute to the development of hammertoe, too. People with diabetes can be at increased risk for complications from a hammertoe. In diabetics, if a toe has a corn or other ulceration, it indicates there is too much pressure on the toes. In those with poor blood flow or neuropathy, these lesions can get infected and lead to the loss of a toe or foot unless shoes are modified.  Symptoms SymptomsHere is a look at some of the symptoms hammertoe can cause. They include hammer-like or claw-like appearance of the toe. Pain when walking or moving the foot. Difficulty moving the toe. Corns may form on top of the toe. Callus may form on the sole of the foot. During the initial stages, you may be able to manually straighten your toe. This is called a Hammer toe flexible hammertoe. But as time passes, the toe will not move as easily and will continue to look like a hammer. Pressure and irritation over the joint can cause a blister to develop and become a corn over time. These corns have the potential to become infected and cause additional symptoms such as redness, bleeding, and difficulty wearing shoes and socks. Corns are the main cause of pain when hammertoes are developing. Diagnosis Although hammertoes are readily apparent, to arrive at a diagnosis the foot and ankle surgeon will obtain a thorough history of your symptoms and examine your foot. During the physical examination, the doctor may attempt to reproduce your symptoms by manipulating your foot and will study the contractures of the toes. In addition, the foot and ankle surgeon may take x-rays to determine the degree of the deformities and assess any changes that may have occurred. Non Surgical Treatment Treatment for a hammertoe usually depends on the stage of the hammertoe and the cause of the condition. If your toe is still bendable, your doctor may suggest conservative care-relieving pressure with padding and strapping, or proper shoes that have a deep toe box and are of adequate length and width. Early intervention can often prevent the need for surgery. Surgical Treatment Surgery to correct for a hammertoe may be performed as a day procedure. There are several different types of procedures that can be used depending on the foot structure and if the deformity is flexible or rigid.  Prevention PreventionPlainly put, most toe deformities are caused by footwear. If you wish to avoid bunions or hammertoes, or works towards reversing them, please choose your footwear that has a low heel, and is wide enough in the toebox to spread you toes. Your podiatrist or therapist can help with the manipulation exercises. Bunion splints are available.
Overview
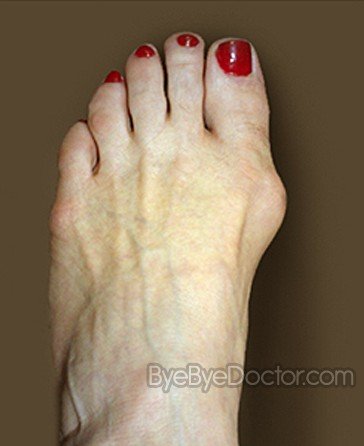 The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe. The classic bunion is a bump on the side of the great toe joint. This bump represents an actual deviation of the 1st metatarsal. In addition, there is also deviation of the great toe toward the second toe. In severe cases, the great toe can either lie above or below the second toe.Causes Bunions result from the long bone in the foot (metatarsal) and the big-toe bone becoming misaligned. The causes are likely to be a combination of genetics, wearing ill-fitting shoes, and the way that we walk or run. Arthritis sufferers are also prone to bunions. Symptoms A bunion, also called a hallux valgus, is a bony prominence on the inside of the big toe, caused by a misalignment of the joint. The overlying skin maybe swollen, red and tender. Bunions are often painful and can limit what shoes you can wear. Diagnosis Your doctor can identify a bunion by examining your foot. Watching your big toe as you move it up and down will help your doctor determine if your range of motion is limited. Your doctor will also look for redness or swelling. After the physical exam, an X-ray of your foot can help your doctor identify the cause of the bunion and rate its severity. Non Surgical Treatment A bunion treatment must address the underlying cause of the deformity, not just the bump (bunion) itself but also the functions of the foot. The up and down motion of the longitudinal arches in the foot. The sideways motion of the transverse arch. Bunion aids effectively treat this underlying foot function while straightening the big toe because the mid-foot strap stabilizes the longitudinal arches and transverse arch. The toe strap gradually and gently pulls the big toe away from the second toe. The metatarsal pad helps align the transverse arch. The hinged splint enables the big toe to flex while walking and adapts to the contour of the foot, especially around the inflamed area of the joint.  Surgical Treatment Depending on the severity of the deformity, this osteotomy can be done either at the end of the metatarsal (a distal osteotomy) or if the deformity is more severe, the osteotomy is performed at the base of the first metatarsal (a proximal osteotomy). One of the more common distal metatarsal osteotomies that is performed is called the chevron osteotomy. Typically a small screw is inserted into the bone to hold the metatarsal head in place and speed up bone healing. Following a chevron osteotomy, walking is permitted in a surgical shoe the next day after surgery and the shoe is worn for approximately three to four weeks before a more comfortable walking/running type shoe is worn. |
